

Study design and sampling
This study utilized a quasi-experimental design with a two-group pretest-posttest approach. Regarding the lack of random assignment in this study, the groups may not be made equal. The participants included patients who had undergone CABG and were followed up after surgery at the outpatient cardiothoracic surgery department of a university hospital in Thailand. Selection for the study was conducted via convenience sampling among patients attending the outpatient department as shown in Fig. 1. The inclusion criteria were: (1) having undergone CABG at least three months prior, and (2) no prior history of CABG. The exclusion criteria encompassed: (1) a history of using substances that may impact sexual function (such as amphetamines, marijuana, cocaine, or heroin) documented in medical records; (2) a previously diagnosed history of depression as recorded by a physician; (3) cognitive impairment identified through a mini-cog screening; and (4) physical disabilities requiring the use of an assistive device for mobility. Patients could also terminate their participation if they were lost to follow-up, could not be contacted, or chose to withdraw from the study.
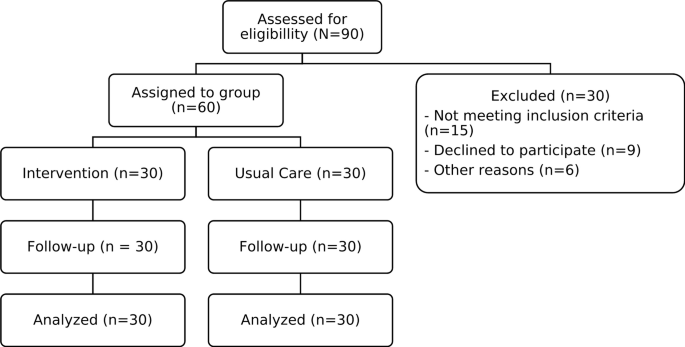
The sample size was determined through a power analysis using the G*Power version 3.1 program, focusing on the provision of sexual education related to sexual quality in patients following CABG. The predictive variables considered in this study were quality of life and sexual knowledge16, with an effect size of 0.78, a test power of 0.80, and a confidence level set at an alpha (α) of 0.05. The initial sample size was 54 subjects, to which 10% was added to account for potential incomplete questionnaires19. Consequently, the required sample size was established at 30 participants per group.
Data collection
The study protocol adhered to the principles outlined in the Declaration of Helsinki. Prior to data collection, written informed consent was obtained from all patients. This study received approval from the Siriraj Institutional Review Board, certifying full compliance (COA No. Si 153/2021). Eligible participants were thoroughly informed about the study’s objectives and asked for their willingness to participate. Once they agreed and signed the consent form, the researcher proceeded to administer the questionnaire, which included the Dementia Screening Assessment (Mini-Cognitive Assessment Instrument, Mini-Cog) and the Sexual Quality of Life Scale.
This study utilized an integrated model of health literacy11. The researcher focused on access to self-concept to develop a program for sexuality education. The research aimed to compare the effects of the sexuality education program on the quality of sexual life between participants and non-participants, employing an experimental design. The goal is to empower individuals undergoing CABG to enhance their understanding and awareness of their sexual quality of life.
The sexual education program has been evaluated by five qualified experts in the fields of cardiology and sexology. The curriculum encompasses the following topics: (1) Factors influencing sexual behavior: including age, mental state, daily habits, and substance use. (2) Readiness for sexual activity: assessing both physical readiness and mental preparedness for engaging in sex. (3) Necessary knowledge about sex: outlining steps to initiate sexual activity at various stages and recommending suitable positions. (4) Guidance on sexual practices: including the importance of consulting a healthcare professional before engaging in sex and the use of appropriate media for exploring sexual eroticism and fantasies. (5) Warning signs and symptoms to be mindful of: identifying harmful signs that may arise during sexual activity. The content has been derived from literature reviews and is suitable for individuals of all genders. The researcher has also completed specialized training in cardiac nursing and clinical sexology.
1. Sexuality education program group
The intervention program comprised two cycles.
First meeting: patient follow up post CABG (30–45 min).
1. Access phase: The researcher initiated a relationship with the patient in a private setting. Open-ended questions were posed to help patients recognize the significance of sexual function, allowing for the expression of their feelings, which took approximately 5–10 min.
“Have you ever received information regarding sexual activity following CABG surgery?”
“What are your thoughts on engaging in sexual activity after CABG surgery?”
2. Understand Phase: The researcher provided comprehensive information about sexual relations for patients post-CABG, facilitating an opportunity for them to learn and comprehend the topic of sexual intercourse after surgery. Patients were encouraged to ask questions and engage in discussions regarding sexual function following CABG.
“What is your understanding of having sex after CABG surgery?”
3. Appraisal phase: The researcher summarized the key issues to enhance knowledge and understanding of sexual relations, revisiting questions, addressing any concerns, and supplying the patient with a sexual education pamphlet.
4. Ongoing monitoring: Throughout the research process, the researcher closely monitored the patient’s complications and scheduled an appointment for the next meeting.
Second meeting: 3 months after the first meeting (30–45 min).
1. Appraisal phase: The researcher reviewed the information provided during the initial meeting concerning patients’ sexual relations in private areas.
2. Application phase: The researcher posed open-ended questions to initiate the discussion:
“What is your perspective on sexual activity after CABG, based on the information you’ve received?”
“What challenges or obstacles have you encountered regarding sexual activity after CABG?”
3. The researcher encouraged patients to ask questions and provided answers throughout the research process:
“If you have any additional questions, please feel free to ask.”
“Should you have any concerns, I invite you to share them so that we can collaboratively explore solutions.”
4. The researcher collected questionnaire data, ensuring that once the questionnaires were completed, the data was securely stored in a sealed envelope.
The intervention program was developed and refined by two cardiovascular nurses with five years of experience in the field. The content validity index was assessed by five experts, including cardiologists, senior cardiovascular nurses, and seasoned cardiovascular nursing researchers, resulting in a content validity index of 0.92.
2. Control group
Following CABG, patients continued to receive standard care and treatment in accordance with established post-CABG guidelines. These guidelines encompass information on behavior modification and postoperative wound care as provided by physicians. Nurses offered guidance on the consistent use of prescribed medications and monitored for any signs and symptoms exhibited by patients prior to their scheduled appointments. Routine follow-up included counseling patients on the importance of quitting alcohol and tobacco use, maintaining a healthy diet, and adhering to exercise regimens essential for cardiac rehabilitation. Recovery progress was assessed every three months, and a sexual quality of life assessment score was evaluated at the conclusion of the three-month follow-up period. Both groups received the same post-care information.
Data analysis
An intention-to-treat analysis was conducted to mitigate selection bias while examining changes in the sexual quality of life among patients. Continuous variables are presented as means and standard deviations (SD) based on their distribution, while categorical variables are shown as frequencies (n) and percentages (%). To compare the baseline characteristics of both groups, Chi-square tests and analyses of variance were employed. The changes in sexual quality of life scores from pretest to posttest were assessed using paired t-tests. Furthermore, independent sample t-tests were utilized to compare posttest sexual quality of life scores between the intervention and control groups. All data analyses were performed using SPSS Statistics version 25 software. A P-value of less than 0.05 was considered statistically significant.
Measures
Dementia screening assessment
The Dementia Screening Assessment, specifically the Mini-Cognitive Assessment Instrument (Mini-Cog), developed by Borson et al. (2000)20 and translated into Thai by Trongsakul et al. (2015)21, serves as a reliable tool for screening patients without cognitive disorders in research involving individuals who have undergone post-CABG (Coronary Artery Bypass Grafting). This single-dimensional scale employs a 5-point system, where word recall accounts for up to 3 points and clock drawing accounts for 2 points. In this study, a cutoff point of ≥ 3 points was used to identify individuals without cognitive impairment.
Demographic data
Demographic data, including gender, age, educational attainment, income, status, duration of relationship, one-night stand sexual experience, last sexual activity, sexual information, disease duration, type of CABG, cardiopulmonary bypass time (CPB) (minutes), body mass index (kg/m2), and current chronic diseases, were used to understand participant characteristics.
Sexual quality of life scale
The symptoms related to sexual quality of life were assessed using the Male Sexual Quality of Life 11-item scale, developed by Abraham et al. (2008)22, and the 18-item Female Sexual Quality of Life scale created by Symonds and Quirk (2005)23. Both scales are single-dimensional and employ a 6-point rating system, ranging from 1 (strongly disagree) to 6 (strongly agree). The questionnaires explore various feelings that patients may experience when contemplating sexual activity, including happiness, frustration, anger, anxiety, shame, or guilt. They also assess feelings related to a perceived loss of masculinity or femininity, as well as satisfaction with the frequency of sexual encounters. The total scores for both questionnaires are converted to a 100-point scale, with higher scores indicating a better sexual quality of life. The validity of these scales has been favorably reported in Oeychanai et al.’s study (Thai version)24, and the overall reliability of the questionnaires has been confirmed, with a Cronbach’s α coefficient of 0.94 for the Male Sexual Quality of Life scale and 0.89 for the Female Sexual Quality of Life scale.
link